ST-Segment Elevation by Current-to-Load Mismatch: An Experimental
and Computational Study
Heart Rhythm 8:111-118, January 2011

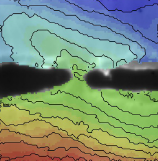
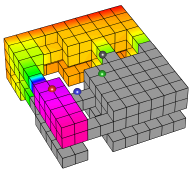
figure 4
links
Paper doi:10.1016/j.hrthm.2010.09.066
Editorial comment doi:10.1016/j.hrthm.2010.09.083
abstract
Background: Recently, we demonstrated [1] that ajmaline caused ST-segment elevation in the heart of an SCN5A mutation carrier by excitation failure in structurally discontinuous myocardium. In Brugada syndrome patients, ST-segment elevation is modulated by cardiac sodium current (INa), transient outward current (Ito) and L-type calcium current (ICaL).
Objective: To establish experimentally whether excitation failure by current-to-load mismatch causes ST-segment elevation and is modulated by Ito and ICaL.
Methods: In porcine epicardial shavings, isthmuses (0.9, 1.1 or 1.3 mm width) were created parallel to the fiber orientation. Local activation was recorded electrically or optically (di-4-ANEPPS) simultaneously with a pseudo-ECG before and after ajmaline application. Intra- and extracellular potentials and ECGs were simulated in a computer model of the heart and thorax before and after introduction of right ventricular structural discontinuities and during varying levels of INa, Ito and ICaL.
Results: In epicardial shavings, conduction blocked after ajmaline in a frequency-dependent manner in all preparation with isthmuses 1.1 mm width. Total conduction block occurred in 3/4 preparations with isthmuses of 0.9 mm vs 1/7 with isthmuses 1.1 mm (p<0.05). Excitation failure resulted in ST-segment elevation on the pseudo-ECG. In computer simulations, subepicardial structural discontinuities caused local activation delay and made the success of conduction sensitive to INa, Ito and ICaL. Reduction of Ito and increase of ICaL resulted in a higher excitatory current, overcame subepicardial excitation failure and reduced the ST-segment elevation.
Conclusions: Excitation failure by current-to-load mismatch causes ST-segment elevation and, like ST-segment elevation in Brugada patients, is modulated by Ito and ICaL
lay abstract
The Brugada syndrome is a combination of changes in the electrocardiogram (ECG) that is associated with a high risk of sudden cardiac death. Brugada syndrome can occur in apparently healthy subjects, and it is especially prevalent in males of 20 to 40 years of age.
A syndrome is a set of symptoms (such as ECG changes) that are often seen together. The Brugada syndrome is defined as a combination of an elevated "ST segment" and negative "T wave" in the ECG, in the absence of structural heart disease or myocardial ischemia. Whether one or more particular diseases underly the syndrome is not yet known. In 30% of cases, genetic mutations have been found whose effects can help to induce the syndrome. Other studies, however, found structural heart disease in 100% of the investigated patients. According to the definition, then, these patients did not have Brugada syndrome. This contradiction occurs because the structural damage is so subtle that it is not detected during clinical investigations, but only on autopsy.
The role of structural damage in Brugada syndrome was not clear. In a previous study, we investigated what role it can play in combination with other factors. Using a combination of experimental and computer model studies, we found that structural damage is necessary to produce the observed ECG changes.
In the current study, we answered two questions raised by our previous work. First, we showed experimentally that structural damage can cause the ECG changes observed in Brugada syndrome. Second, we showed with computer simulations that certain types of drugs can influence the ECG changes, and may trigger arrhythmia.
funding
This work was supported by The Netherlands Heart Foundation (2008B062 [Dr. Coronel]) and by the Interuniversity Cardiology Institute of the Netherlands. Computational resources for this work were provided by the Réseau québécois de calcul de haute performance (RQCHP).